

The best doctors give the least medicine.
- Benjamin Franklin
The demonisation of cholesterol
Cholesterol has been demonised as the major contributing factor in causing heart disease. Here’s the theory behind this:
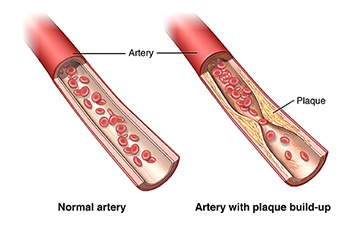
- most heart attacks are caused by blockage due to the build up of plaque in the coronary arteries that supply the heart
- cholesterol is a major component of that plaque
- this plaque build-up eventually cuts off the blood supply to certain areas of the heart, causing oxygen deficiency, pain (angina) and ultimately a heart attack.
So it stands to reason that cholesterol, as it is always present in arterial plaque, must be a major concern and therefore reducing it is a good idea. You may have heard about good and bad cholesterol, High-Density Lipoprotein (HDL) and Low-Density Lipoprotein (LDL). HDL is the good stuff because it picks up excess cholesterol and takes it back to the liver, whereas LDL is the stuff that carries cholesterol to the arterial blockage. HDL and LDL are not actually cholesterol but proteins that act as transport mechanisms for cholesterol to and from the liver.
One of the best analogies I saw on this subject was this: “blaming cholesterol for causing heart attacks is like blaming firemen for causing fires, as they are always there at the scene.” The cholesterol is actually there due to the body’s intelligent response to damaged tissue, it’s there to heal, not to harm.

In fact, cholesterol is vital to the process of building healthy cells, for hormone production and for producing cortisol, which is the body’s own anti-inflammatory agent. It’s the precursor to the production of vitamin D and it’s a powerful antioxidant that protects against cancer and ageing. Given that cholesterol is so vital to the body, why would we want to suppress its production? Maybe the body’s producing too much of it? Well, that supposes that your body is not intelligent and doesn’t know what it’s doing. The production of cholesterol is the body’s natural response to dealing with inflammation. In other words, it’s trying to heal tissue damage.
The real cause of atherosclerosis
So what causes this damage or “Atherosclerosis”, the medical term used to describe the narrowing of arteries from plaque? If this blockage is caused by cholesterol, then why don’t our veins and capillaries get clogged up? Atherosclerosis only occurs in arteries as it is the muscular layer in arterial walls that is getting damaged by free radicals, sourced from the polyunsaturated oils in our diet.
These are the vegetable oils that we were told to switch to as they are “healthier” than saturated fats. The higher ratio of Omega 6 to Omega 3 that is in most vegetable oils has an inflammatory effect on the body, unlike fish oil which has a higher level of Omega 3. It is increased consumption of these oils that is causing the free radical damage to the arterial walls. We need to be reducing the stuff that causes the damage not the stuff that is there to repair it – only that way will our bodies get the chance to recover.
So, how do Statins reduce cholesterol in the body? Cholesterol is produced by the liver, which is a remarkable organ that produces so many chemicals, enzymes and nutrients in a vastly complex branch of reactions. Imagine that the liver is a tree where the end of each twig is a vital compound for the body, such as cholesterol. Statins don’t prune that single twig, they actually cut further into the branch, reducing other vital “twigs”. One such twig is Coenzyme Q10 (COQ10). COQ10 is used for energy production by every cell in your body. Without it your muscles will weaken, including the heart which is a major muscle. Another “twig” is Vitamin K2, which protects arteries from calcification and removes calcium from where it shouldn’t be in soft tissues.
Relative Risk v. Absolute Risk
Statins became such big business, partly down to the cholesterol myth (blaming the fire fighters) but also partly due to how the risk is presented. When discussing risk reduction of disease due to medication or the risk of unwanted side-effects from that medication it is important to understand the difference between Relative Risk Reduction (RRR) and Absolute Risk Reduction (ARR). Let’s take an example to illustrate the difference. One study showed that for high-risk patients with Type 2 Diabetes, taking 10mg of Atorvastatin every day for 4 years reduced the risk of that patient experiencing a stroke by 48%.
That’s an impressive statistic and would convince many people in a 10 minute consultation with their GP. However, the real figures behind it tell a different story. The numbers show that risk of suffering a stroke is actually reduced from 28 in 1000 people down to 15 in 1000. In other words, by taking the drug, 13 people in 1000 were prevented from having a stroke. In Absolute Risk Reduction terms that is only 1.3%. Compare that to the 48% quoted in RRR terms! Another way to look at it is that most people do not benefit.
There is a tendency to report the benefits of drugs in terms of Relative Risk Reduction, whilst harmful side-effects are reported in absolute terms. For example, if treatment A reduces the risk of developing disease from 10 to 7 in 1000 people, but increases the risk of harmful effect B from 7 to 10 in 1000, medical journal article tends to report the benefit as a 30% risk reduction but the harmful side affect has an increase of 3 in 1000 or 0.3%. Is that cheating? I couldn’t possibly comment. A study showed that one third of the articles in medical journals published in Lancet, BMJ (British Medical Journal) and JAMA (Journal of the American Medical Association), between 2004 and 2006 did this.
Statin side-effects
So what are the side effect risks of statins? One popular Statin, Lipitor, has a list of side-effects that includes: headache, joint pains, mild muscle pain, constipation, diarrhoea, stomach pain or indigestion, mild nausea, mild skin rash, sleep problems, jaundice, dark urine, confusion, muscle wasting, liver and kidney problems.
Take a look here and see for yourself. The effects are such that 58% of patients stop taking them within a year, mostly because they experience muscle pain and fatigue.

I remember discussing this with one of my clients who was taking Statins. I sent her some links to videos which explained what I’ve outlined in this blog. Several months later she told me that she had decided to stop taking Statins on the basis of the evidence outlined in those videos. She explained that after 3 months (which is how long it takes to start to recover from Statin side-effects) she realised that she could walk downstairs without feeling like an old woman.
When she next saw her GP it was with much trepidation as she told him that she had stopped taking her Statin prescription. He tested her cholesterol levels and found that they were within what was considered a healthy range; so he removed the Statins from her repeat prescriptions. I’m convinced that the cholesterol reduction was due to her changes in diet by virtually eliminating sugar and grain-based vegetable oils.
She then reported that her husband, who was also taking Statins and suffering from muscle pains, decided to stop taking them, to see what would happen. Sure enough the muscle aches went away. He then resumed the Statins and those aches returned.
Be fully informed
As a Kinesiologist I am a complementary health practitioner and as such I cannot, and would not, advise anyone to stop taking any prescribed drugs. But I think everyone should be completely aware of the facts so that they can take a fully informed decision before starting treatment with drugs. That includes understanding the real benefits in terms of disease risk reduction and side-effects of any medication.
When you next have a discussion with your GP about whether a drug, such as Statins, would be beneficial, make sure that they can explain these risks to you in absolute terms. Ultimately it is your decision about what medical treatment to receive and whether you believe the benefits really outweigh the risk.